EXAMINATION:
CT LUMBAR SPINE Clinical History:
Back pain with radiculopathy Comparison:
No prior study for comparison.
Technique:
Unenhanced helical acquisition performed through the lumbar region with multiplanar 2D reformats and dedicated lumbar disc assessment.
Findings: Normal spinal alignment.
No destructive lesions. L1-2:
No focal disc protrusion, spinal canal or foraminal stenosis detected.
Normal facet joints. L2-3:
No focal disc protrusion, spinal canal or foraminal stenosis detected.
Normal facet joints. L3-4:
No focal disc protrusion, spinal canal or foraminal stenosis detected.
Normal facet joints. L4-5:
No focal disc protrusion, spinal canal or foraminal stenosis detected.
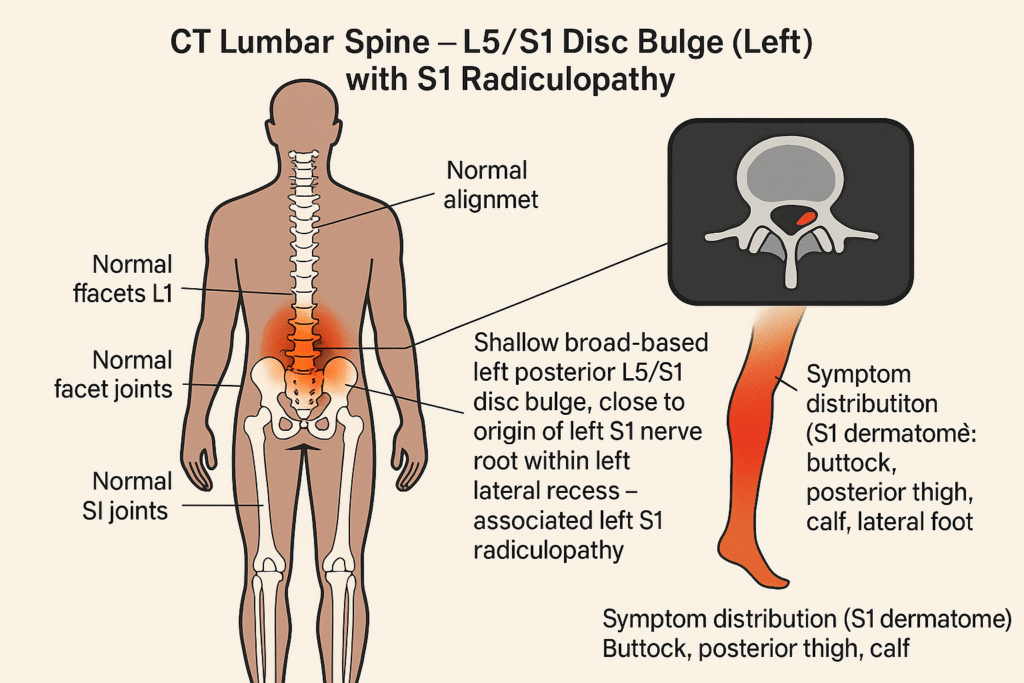
Normal facet joints. L5-S1: There is a shallow left posterior L5/S1 disc bulge which is close to the origin of the left S1 nerve root within the left S1 lateral recess? Associated with left S1 radiculopathy.
Normal facet joints.
Normal appearances of the sacroiliac joints
CONCLUSION:
Shallow broadbased left posterior L5/S1 disc bulge close to the origin of the left S1 nerve root?
Associated with left S1 radiculopathy Other disc levels appear normal Dr Mark Keen Queensland X-Ray
CT Lumbar Spine — Clean Radiology-Style Summary
Study: CT Lumbar Spine
(unenhanced helical with multiplanar reformats)
Comparison: None available at time of scan
Alignment/Bones:
Normal alignment; no destructive bony lesions
Sacroiliac joints: Normal
Level-by-level
- L1–2: No disc protrusion. No canal or foraminal stenosis. Facets normal.
- L2–3: No disc protrusion. No canal or foraminal stenosis. Facets normal.
- L3–4: No disc protrusion. No canal or foraminal stenosis. Facets normal.
- L4–5: No disc protrusion. No canal or foraminal stenosis. Facets normal.
- L5–S1: Shallow left-posterior disc bulge in the left lateral recess, close to the origin of the left S1 nerve root. Facets normal.
Impression / Conclusion
- Shallow broad-based left-posterior L5/S1 disc bulge, close to the left S1 nerve root, associated with left S1 radiculopathy.
- All other lumbar levels appear normal.
CT in Plain English
- Your lower spine alignment and joints look normal overall.
- At L5/S1, the disc sticks out a little to the left at the back.
- That small bulge sits very near the left S1 nerve,
- which can irritate that nerve and cause S1-type leg symptoms (buttock → back of thigh → calf → outer/sole of foot).
- The rest of the discs and nerve exit spaces look normal on CT
- Patient Storyline / History of Present Illness (HPI)
- As of: 16 Aug 2025
- Timeline (≈12 months since injury)
- Aug 2024 — Work injury:
Sudden onset low-back pain with radiation to both legs, - left leg 4–6× worse than right leg. Continued working despite persistent pain.
- Aug–Oct 2024 — Ongoing but working:
Daily private deep-tissue massage to complete work shifts. Describes dragging of the left leg, Pain constant; worsened by activity and driving. sleep, walking normal activity - Late Oct–Early Nov 2024 — Rapid escalation:
Increasing leg “giving way” episodes on the way to and at work. Later assessment identified hip bursitis as a contributing pain source. Marked decline in mobility. - 04 Nov 2024 — Acute crisis:
Woke bed-bound, unable to move more than an inch.
Unable to walk, drive (manual car), work, or manage flat ground or stairs.
By ~12:00pm excruciating, uncontrolled pain, vocal distress/screaming reported. ambulance was called - Wed 06 Nov 2024 — CT lumbar spine performed (Queensland X-Ray):
(Results documented separately on the CT summary page.) - Post-CT — MRI arranged (compared to CT 06 Nov 2024):
(Results documented separately on the MRI summary page.) - Symptoms (since onset)
- Low-back pain constant; flares with movement.
- Radicular features both legs, left»right; episodes of deep itch/tingle/pain.
- Functional losses during peak:
- unable to bend hip/knee/back, unable to walk or climb stairs, unable to drive, unable to work.
- Falls/near-falls due to leg “giving way.”
- Current status (as of 16 Aug 2025)
- Ongoing low-back pain with intermittent left-sided leg symptoms. nerve problems still present.
- Engaged in conservative care (manual therapy/exercise as tolerated).
- Activity restrictions in place: avoids rotation/side-bending under load; uses neutral-spine positions; limits lifting to light loads only.
- Work capacity limited by pain flares and mobility.